Carpal Tunnel Syndrome
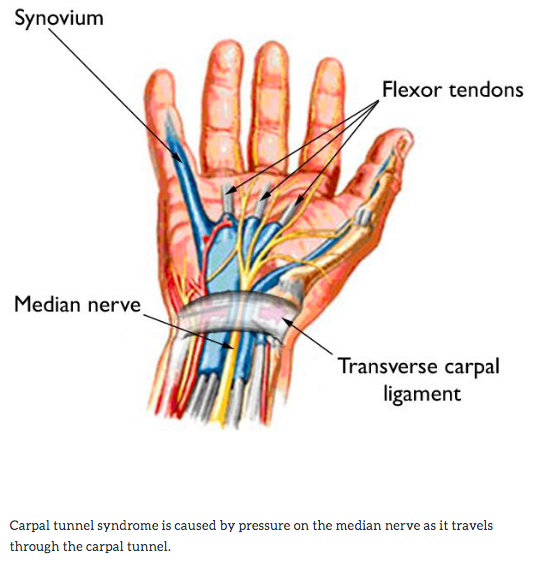
Carpal tunnel syndrome is a common condition that causes pain, numbness and tingling in the hand and arm. The condition occurs when one of the major nerves to the hand – the median nerve – is squeezed or pinched as it travels through the wrist. There is a space in the wrist called the carpal tunnel where the median nerve and nine tendons pass from the forearm into the hand (Figure 1). Carpal tunnel syndrome happens when the tunnel becomes narrowed or when tissues surrounding the flexor tendons swell, putting pressure on the median nerve.
Causes
Most cases of carpal tunnel syndrome are caused by a combination of factors. Studies show that women and older people are more likely to develop the condition.
Other risk factors for carpal tunnel syndrome include:
- Heredity. This is likely an important factors. The carpal tunnel may be smaller in some people of there may be anatomic differences that change the amount of space for the nerve – and these traits can run in families.
- Repetitive hand use. Repeating the same hand and wrist motions or activities over a prolonged period of time may aggravate the tendons in the wrist, causing swelling that puts pressure on the nerve.
- Hand and wrist position. Doing activities that involve extreme flexion or extension of the hand and wrist for a prolonged period of time can increase pressure on the nerve.
- Pregnancy. Hormonal changes during pregnancy can cause swelling.
- Health conditions. Diabetes, rheumatoid arthritis and thyroid gland imbalance are conditions that are associated with carpal tunnel syndrome.
Signs and Symptoms
Symptoms of this condition can include:
- Pain or tingling that may travel up the forearm toward the shoulder
- Numbness, tingling, burning, and pain – primarily in the thumb and index, middle, and ring fingers
- Weakness and clumsiness in the hand – this may make it difficult to perform fine movements such as buttoning your clothes
- Tendency to drop things due to weakness, numbness, or a loss of proprioception (awareness of where your hand is in space)
In most cases, the symptoms of carpal tunnel syndrome begin gradually – without a specific injury. Many patients fine that their symptoms come and go at first. However, as the condition worsens, symptoms may occur more frequently or may persist for longer periods of time.
Night-time symptoms are very common. Because many people sleep with their wrists bent, symptoms may awaken you from sleep. During the day, symptoms often occur when holding something for a prolonged period of time with the wrist bent forward or backward, such as when driving, using a phone, or reading a book or newspaper. Many patients find that moving or shaking their hands helps relieve their symptoms. In severe cases, sensation and strength may be permanently lost.
Diagnosis
During your evaluation, your doctor will talk to you about your general health and medical history and will ask about your symptoms.
He or she will carefully examine your hand and wrist and perform a number of physical tests. During these tests, your doctor will:
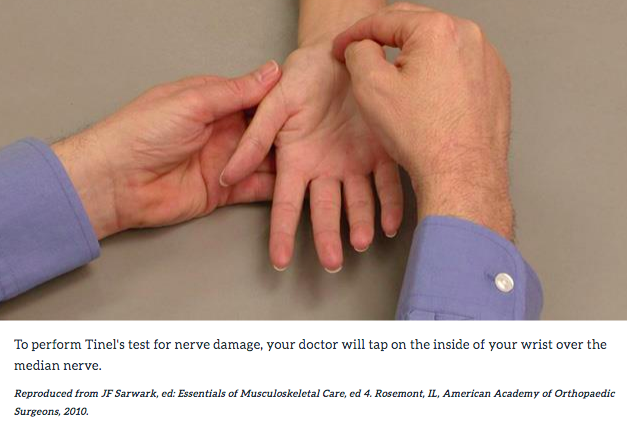
- Press down or tap along the median nerve at the inside of your wrist to see if it causes any numbness or tingling in your fingers (Tinel sign). (Figure 2).
- Bend and hold your wrists in a flexed position to test for numbness or tingling in your hands
- Test sensitivity in your fingertips and hands by lightly touching them with a special instrument when your eyes are closed.
- Check for weakness in the muscles around the base of your thumb. Look for atrophy in the muscles around the base of your thumb. In severe cases, these muscles may become visibly smaller.
Tests
Electrophysiological tests. These tests will help your doctor measure how well your median nerve is working and help determine whether there is too much pressure on the nerve. The tests will also help your doctor determine whether you have another nerve condition such as neuropathy, or other sites of nerve compression that might be contributing to your symptoms.
Electrophysiological tests may include:
- Nerve conduction studies. These tests measure the signals traveling in the nerves of your hand and arm and can detect when a nerve is not conducting its signal effectively. Nerve conduction studies can help your doctor determine how severe your problem is and help to guide treatment.
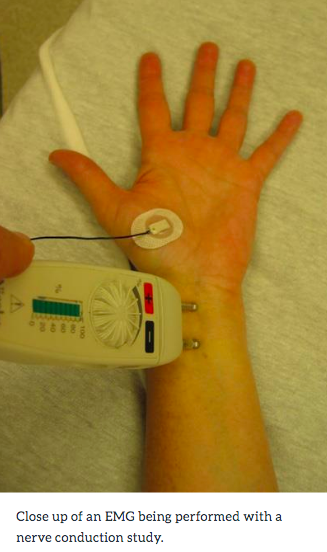
- Electromyogram (EMG). An EMG measures the electrical activity in muscles. EMG results can show whether you have any nerve or muscle damage. (Figure 3).
Ultrasound. An ultrasound uses high-frequency sound waves to help create pictures of bone and tissue. Your doctor may recommend an ultrasound of your wrist to evaluate the median nerve for signs of compression.
X-rays. X-rays provide images of dense structures, such as bone. If you have limited wrist motion or wrist pain, your doctor may order x-rays to exclude other causes for your symptoms, such as arthritis, ligament injury, or a fracture.
Magnetic resonance imaging (MRI) scans. These studies provide better images of the body’s soft tissues. Your doctor may order an MRI to help determine other causes for your symptoms or to look for abnormal tissues that could be impacting the median nerve. An MRI can also help your doctor determine if there are problems with the nerve itself—such as scarring from an injury or tumor.
Treatment
Although it is a gradual process, for most people carpal tunnel syndrome will worsen over time without some form of treatment. For this reason, it is important to be evaluated and diagnosed by your doctor early on. In the early stages, it may be possible to slow or stop the progression of the disease.
Nonsurgical Treatment
If diagnosed and treated early, the symptoms of carpal tunnel syndrome may often be relieved without surgery. Some treatment options are:
- Bracing or splinting. Wearing a brace or splint at night will keep you from bending your wrist while you sleep. Keeping your wrist in a straight or neutral position reduces pressure on the nerve in the carpal tunnel. It may also help to wear a splint during the day when doing activities that aggravate your symptoms.
- Nonsteroidal anti-inflammatory drugs (NSAIDs). Medications such as ibuprofen and naproxen can help relieve pain and inflammation.
- Activity changes. Symptoms often occur when your hand and wrist are in the same position for too long—particularly when your wrist is flexed or extended.
If your job or recreational activities aggravate your symptoms, changing or modifying these activities can help slow or stop progression of the disease. In some cases, this may involve making changes to your work site or work station.
- Nerve gliding exercises. Some patients may benefit from exercises that help the median nerve move more freely within the confines of the carpal tunnel. Specific exercises may be recommended by your doctor or therapist.
Click here for a handout for nerve gliding exercises for carpal tunnel syndrome
- Steroid injections. Corticosteroid, or cortisone, is a powerful anti-inflammatory agent that can be injected into the carpal tunnel. Although these injections often relieve painful symptoms or help to calm a flare up of symptoms, their effect is sometimes only temporary. A cortisone injection may also be used by your doctor to help diagnose your carpal tunnel syndrome.
Surgical Treatment
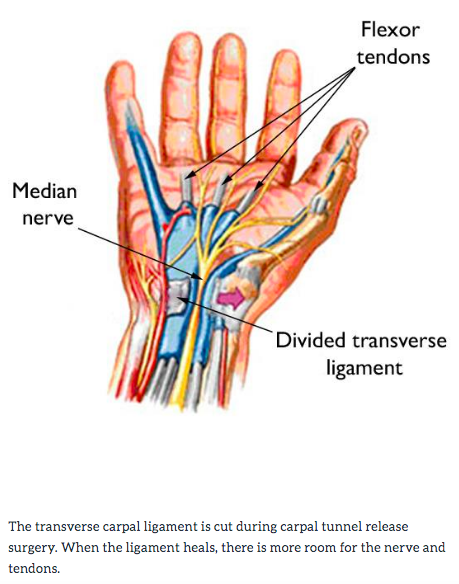
When symptoms are severe or do not improve, surgery may be needed to make more room for the nerve. The surgical procedure performed for carpal tunnel syndrome is called a “carpal tunnel release.” Pressure on the nerve is decreased by cutting the ligament that forms the top of the tunnel on the palm side of the hand (Figure 4). This increases the size of the tunnel and decreases pressure on the median nerve. In most cases, carpal tunnel surgery is done on an outpatient basis. The surgery can be done under general anesthesia, which puts you to sleep, or under local anesthesia, which numbs just your hand and arm. In some cases, you will also be given a light sedative through an intravenous (IV) line inserted into a vein in your arm.
Immediately following surgery, you will be encouraged to elevate your hand above your heart and move your fingers to reduce swelling and prevent stiffness.
You should expect some pain, swelling, and stiffness after your procedure. Minor soreness in your palm may last for several weeks to several months.
Grip and pinch strength usually return by about 2 to 3 months after surgery. If the condition of your median nerve was poor before surgery, grip and pinch strength may not improve for about 6 to 12 months.
You may have to wear a splint or wrist brace for several weeks. You will, however, be allowed to use your hand for light activities, taking care to avoid significant discomfort. Driving, self-care activities, and light lifting and gripping may be permitted soon after surgery.
Your doctor will talk with you about when you will be able to return to work and whether you will have any restrictions on your work activities.